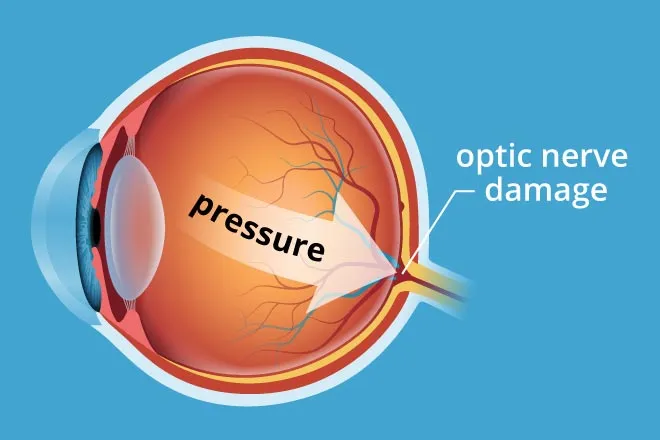
Acute angle closure glaucoma is a type of primary glaucoma (wherein there is no obvious systemic or ocular cause) in which rise in intraocular pressure occurs due to blockage of the aqueous humour outflow by closure of a narrower angle of the anterior chamber. Acute angle-closure glaucoma is an urgent but uncommon dramatic symptomatic event. It is a medical emergency. Glaucoma is not a single disease process but a group of disorders characterized by a progressive optic neuropathy resulting in a characteristic appearance of the optic disc and a specific pattern of irreversible visual field defects that are associated frequently but not invariably with raised intraocular pressure (IOP).

The angle refers to the angle between the iris and the cornea in the anterior chamber which can become structurally obstructed. By definition, primary glaucoma is not associated with known ocular or systemic disorders and usually affect both eyes. Secondary glaucoma is associated with ocular or systemic disorders and are often unilateral. The commonly accepted range for intraocular pressure is 10-22 mm Hg. There are three factors that affect intraocular pressure: the rate of production of aqueous humor by the ciliary body, the resistance to aqueous outflow through the trabecular meshwork and Schlemm’s canal, and the episcleral venous pressure. In acute angle closure glaucoma, intraocular pressure increases rapidly due to outflow obstruction of the aqueous humor. There are several factors leading to the obstruction in acute angle closure glaucoma, but the major predisposing factor is the structural anatomy of the anterior chamber leading to a shallower angle.
Understanding the Process
Aqueous humour (a transparent, low protein containing fluid) is continuously secreted by the ciliary epithelium which provide structural support to the lens. This watery fluid is present in both the anterior and posterior chambers of the eye and drains through a sieve-like trabecular meshwork which is located in the angle between the cornea and the iris. Finally, it is drained out of the eye occurs via the canal of Schlemm into the epistler vein or intrascleral venous plexus terminating in the ocular veins. Under angle closure glaucoma there is angle closure with pupillary block under which acute angle closure glaucoma falls. With closed angle glaucoma, a primary hypermetropic anatomical defect (such as weakened ciliary muscles, naturally small eyes, narrow angle or thick lens) in the absence of an identifiable
secondary cause, results in the pupil compressing the drainage canal between the iris and cornea. Compression and narrowing of the canal reduces or obstructs the outflow of aqueous humour in
passing through the pupil, therefore accumulating in the anterior chamber. Primary angle closure glaucoma (PACG) is less common than POAG and accounts for approximately a third of all cases.

Symptoms
Symptoms of closed angle glaucoma depend on the degree of angle closure and in some instances may resolve spontaneously; in which case it may become chronic. In established disease, vision loss is severe and permanent. There is pain. Typically, acute attack is characterised by sudden onset of very severe pain in the eye which radiates along the branches of 5th nerve. There is nausea, vomiting and prostrations which is frequently associated with pain. Also, there is rapid progressive impairment of vision, redness, photophobia and lacrimation develop in all cases. About 5 percent patients give history of typical previous intermittent attacks of subacute angle-closure glaucoma.

Who is at Risk?
Risk factors for angle closure glaucoma include older age (> 60 years), female gender, Asian
ethnicity, hyperopia and a positive family history.11 Attacks occur more frequently at night when diminished light cause mydriasis and narrowing of the angle.12 Unexpected closure (acute angle closure glaucoma, AACG) of the anterior chamber angle due to pupillary block may result in a sudden rise in IOP. It constitutes a medical emergency, since permanent blindness and irreversible damage to the optic nerve may occur.

Management
The treatment of acute angle-closure glaucoma (AACG) consists of IOP reduction, suppression of inflammation, and the reversal of angle closure. Once diagnosed, the initial intervention includes acetazolamide, a topical beta-blocker, and a topical steroid. Patients may also be placed in a supine position to allow the lens to move away from the anterior chamber to help restore of the flow of aqueous humor. Laser peripheral iridotomy (LPI), performed 24-48 hours after IOP is controlled, is considered the definitive treatment for AACG. Furthermore, LPI may be offered prophylactically to individuals anatomically predisposed to AACG if identified before the first acute attack.


What is @bettervision about?
@bettervision is is a project initiated by @nattybongo and friends to give back to the society the knowledge and skill acquired through the Optometric Studies in Kwame Nkrumah University of Science and Technology, Ghana.It is an outreach system where we visit the less privileged communities to offer free eye screening services and education to the people within the community
AIMS AND OBJECTIVES
To reduce or prevent vision loss through diseases such as glaucoma, cataract and refractive errors.
To enlighten the majority of the Ghanaian population about the importance of proper visual care.
To conscientize people on the need for regular eye checks
To get more people to have their wards screened within the Critical periods of a Child’s Vision Development; thus from ages 3 to till about 10 years.
To help the blind and people with low vision live a better life within the society through education of the general public to stop stigmatization.
To help in the fight of extreme poverty that puts the health of people at risk
Our greatest gratitude goes to @fundition @adollaraday @surfyogi @girlsfoundation @bleepcoin @ackza @indigoocean @nanzo-scoop @steemstem @demotruk @pennsif @steem-ambassador @kasho and @wafrica for helping to make the aims and objectives of @bettervision a reality.

shirt.jpg](https://images.ecency.com/p/3jpR3paJ37V8JxyWvtbhvcm5k3roJwHBR4WTALx7XaoRovbdkGwm8sDfo9UUXEuNZXBMC1kdmJ6coMxZnzE8tqnHbG5dNEHKxuT43r9nisaaZ4NderHKyDtCXn8wp1tG6F6zi.png?format=match&mode=fit)